
by Kevin Schofield
This week’s “long reads” has just one topic, but two related papers worth reading. Scientists now have a very good idea why older people tend to have more serious cases of COVID-19. And there are some very important implications of this, which we can take action on today.
Back in March, epidemiologists studying the spread of the coronavirus around the globe noticed two unusual things. First, the older you are, the more likely you are to have serious complications from contracting COVID-19; conversely, kids and young adults tend to have very mild cases. In fact, there seems to be a “pivot point” right around age 50, above which the percentage of people with serious cases skyrockets.
Second, there is wide variation across countries in the fatality rate for COVID-19, with several (including Hong Kong, Madagascar, North Korea, Turkmenistan, the Cook Islands, and South Korea) having unusually low rates and others (including Italy and Belgium) having particularly high ones.
The scientists found something that connects these two observations: the MMR vaccine, or more generally, the collection of widely-used vaccines to inoculate individuals against measles, mumps, and rubella. The MMR II vaccine, used around the world, was introduced around 1971. It’s typically given in two doses: the first to babies at around 12 months of age, and the second at age 4 to 5. That means in many developed countries anyone under the age of about 50 has been vaccinated with MMR. But many developing countries historically have not administered the MMR vaccine to all children — though some have in recent years, for instance at the onset of a major measles outbreak.
The epidemiologists found that countries with high rates of MMR vaccination tend to have lower rates of serious cases of COVID and fewer fatalities. The fact that the immunity we gain from a vaccination can tend to fade with time explains why children, who have been recently immunized for MMR, tend to be largely unaffected by COVID, while older generations are hit harder. And the COVID “pivot point” at around age 50 lines up nearly perfectly with the year that MMR vaccinations were first introduced.
There’s more evidence for the connection. You may recall the U.S.S. Roosevelt, which had an outbreak of over 1,100 sailors on-board who tested positive for COVID last spring. But it had very few deaths or hospitalizations. It turns out that the U.S. military gives all new recruits MMR vaccinations upon enlistment, regardless of their prior vaccination history.
Hong Kong instituted a mass MMR vaccination campaign for children in 1997, and in 2019 held another free MMR vaccination campaign for all adult workers, airport staff, foreign domestic helpers, and many other adults. To-date, Hong Kong (population 7.5 million) has only had 5,867 confirmed COVID cases and 108 deaths. Washington State — same population — has had 151,000 cases and 2,690 deaths. Iran had a massive MMR vaccination effort in 2003, inoculating 33 million people, but each received only one of the two doses in the full vaccination regimen; Iran is on the low end for cases, but in the middle of the range for fatalities.
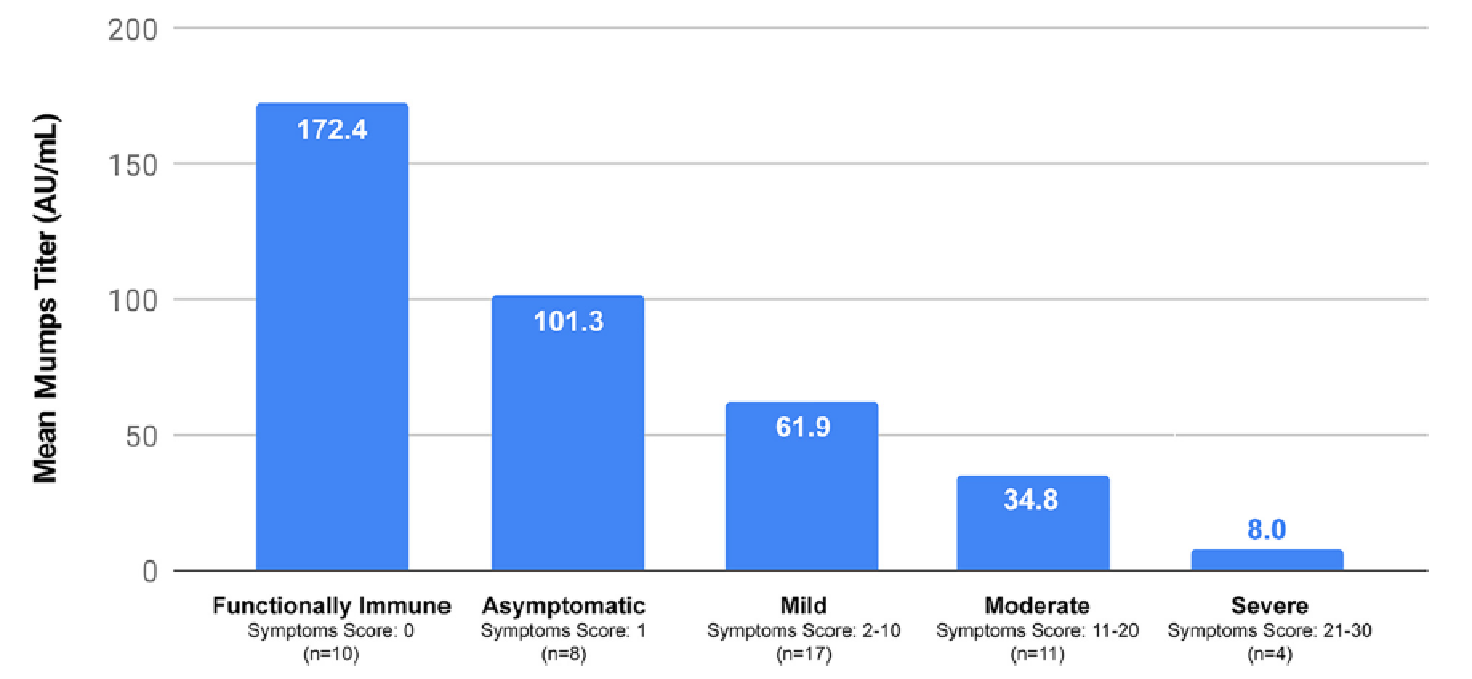
Late last week, a new study was published following up on the observed connection between COVID and MMR. In the study, researchers checked the levels of mumps antibodies in the bloodstream of people who had tested positive for COVID-19. They found that among the people who had received an MMR vaccine, those with higher levels of mumps antibodies (or their “mumps titer”) had less severe cases of COVID (and vice versa). But among another group who had not been vaccinated but had likely acquired immunity through exposure to the disease itself, they found no connection between the level of mumps antibodies and COVID symptoms.
This tells us that something in the MMR vaccine is creating a resistance to COVID, and the more recently someone was vaccinated with it, the higher their resistance. It matches up well with recent research showing that people with a high “viral load” of COVID at the point they are hospitalized tend to fare poorly, and other research indicating that “dosing” is important: People who get a large exposure to COVID seem to have more severe cases. The amount of the coronavirus in your body seems to be strongly linked to severity, and everything that reduces the exposure and/or viral load — mask wearing and social distancing, quick immune reactions, and potentially antiviral medicines or “antibody cocktails” like the one President Trump was given — leads to milder cases.
Now there are some important caveats here. First, this new research needs to be replicated by other teams of scientists before we can thoroughly trust it: It’s a new, first result, and it isn’t science unless and until it can be replicated. Second, we don’t know exactly what it is in the MMR vaccine that is generating an immune response against COVID, let alone what that immune response actually is. The human body’s immune system is a collection of about a dozen different mechanisms, many of which can be “trained” by vaccines to fight off disease. It’s difficult to trace back the source of the COVID resistance in the MMR vaccine.
This research also doesn’t tell us anything about transmissibility of COVID by people with the MMR vaccine. It’s already well established that people with no symptoms, or just mild ones, can still be significant vectors for spreading COVID. And since a large portion of the U.S. population, including millennials, has been vaccinated with MMR, there’s at least anecdotal evidence that the MMR vaccine doesn’t stop people from being contagious. If it did — or if we found that people who were immunized within, say, two years, were effectively immune to COVID — then we might be able to get preschools and kindergartens reopened sooner. But we don’t know that now, and it’s likely that the COVID vaccines will arrive before we can figure that out in the short term.
And before you rush off to your doctor to try to get an MMR shot, there are a few things you should keep in mind. First, there is a limited supply, probably further constrained by the extent to which vaccine production facilities are currently dedicated to COVID. That means if there is suddenly a mad rush for adults to get MMR vaccines, there won’t be enough for the kids who would normally get them — increasing their exposure (not to mention their families and classmates) not only to COVID but also to mumps, measles, and rubella. Moreover, while there is plenty of data on the safety of MMR vaccines for young children, and lots of precedent for giving it safely to teenagers and young adults, there is much less data on the safety and effectiveness of MMR vaccines for older adults. And there is no data on what happens when an adult receives MMR and COVID vaccines within a short period of time.
That said, if you’re a teenager or a young adult, you should definitely check your vaccination history to make sure you’re up-to-date on your MMR vaccination, and if you’re not, then contact your healthcare provider; likewise, if you’re a parent, check your kids’ immunization records. These days schools require MMR vaccinations, so most kids are up-to-date, but it’s still worth checking. While the CDC is now saying that the first COVID vaccine distributions will be in the next few weeks, they likely won’t have scaled up availability to everyone until around April.
One of the ongoing worries about the new COVID vaccines is that, like the flu shot, they won’t confer long-term immunity. But this new research on the MMR vaccine suggests that its immunity to COVID might persist (in fact, has persisted) for decades. Don’t be surprised if there is substantially more research on the MMR vaccine and COVID in the coming months that might lead to more robust vaccines.
A last note: the MMR vaccine has been a frequent target of anti-vaxxers. Their arguments questioning the safety of the MMR vaccine, or suggesting that it causes autism, have been thoroughly and repeatedly debunked.
MMR Vaccine Appears to Confer Strong Protections from COVID-19 (March/April 2020)
Analysis of Measles-Mumps-Rubella (MMR) Titers of Recovered COVID-19 Patients (November 2020)
Kevin Schofield is a freelance writer and the founder of Seattle City Council Insight, a website providing independent news and analysis of the Seattle City Council and City Hall. He also co-hosts the “Seattle News, Views and Brews” podcast with Brian Callanan, and appears from time to time on Converge Media and KUOW’s Week in Review.
Before getting into journalism Kevin worked at Microsoft for 26 years, including 17 in the company’s research division. He has twin daughters, loves to cook, and is trying hard to learn Spanish and the guitar.
Featured image is attributed to Silvision under a Creative Commons 2.0 (CC BY-ND 2.0) license.